We are excited to announce our new course, “Combination Antibiotic Therapy for Treatment of Lyme Disease.” This course is designed for medical professionals seeking to deepen their understanding of Lyme disease treatment. It centers around the groundbreaking study conducted by Dr. Monica Embers, Director of Vector-Borne Disease Research at Tulane University. To provide a comprehensive overview, we invited Dr. Embers to answer key questions about her study on combination antibiotic therapy.
Q: Dr. Embers, could you explain the main goals of your study?
Dr. Embers: Certainly! Our primary goals were to distinguish between antibiotic tolerance and resistance in Lyme disease, demonstrate persistence via tolerance by the Lyme disease spirochete, and evaluate the efficacy of combination therapy versus monotherapy in both animal models and humans.
Q: What are the key findings regarding antibiotic tolerance and resistance?
Dr. Embers: We found that Lyme disease bacteria, Borrelia burgdorferi, can become tolerant to antibiotics, meaning they can survive prolonged exposure without developing resistance. This tolerance contributes to the persistence of infection despite standard antibiotic treatment.
Q: How effective is combination therapy compared to monotherapy?
Dr. Embers: Our study showed that combination therapy – using multiple antibiotics – is more effective in targeting different forms of the Lyme disease bacterium, including dormant forms. This approach seems more successful in eradicating the infection compared to monotherapy.
Q: Can you discuss the prevalence of Post-Treatment Lyme Disease (PTLD) and its causes?
Dr. Embers: Yes, PTLD is a condition where symptoms persist even after antibiotic treatment. Our study suggests that the prevalence of PTLD might be higher than previously estimated. The causes could include inflammatory responses triggered by remnants of the bacteria, ongoing infection, or autoimmune responses.
Q: What insights did your research provide regarding the standard treatment guidelines for Lyme disease?
Dr. Embers: We found discrepancies between different guidelines, such as those from IDSA and ILADS, particularly concerning the duration and choice of antibiotics. Our research suggests that extended and combination therapies might be more effective, especially for patients with persistent symptoms.
Q: How do you see the future of Lyme disease treatment evolving based on your study?
Dr. Embers: Our study paves the way for more comprehensive treatment approaches, emphasizing the need for combination therapy. Future clinical trials should focus on these approaches to develop more effective and sustained treatments for Lyme disease, especially for those with PTLD.
Q: Lastly, what message do you have for patients currently struggling with Lyme disease?
Dr. Embers: It’s important to advocate for your health. If you’re experiencing persistent symptoms, seek medical advice and discuss the possibility of extended or combination antibiotic therapy. Stay informed and involved in your treatment process.
Thank you, Dr. Embers, for your insightful answers and for your dedication to Lyme disease research. Your study offers hope and a new direction in the fight against this challenging disease.
Watch the Course Here
The Invisible Education Initiative, funded by the Montecalvo Foundation, provides free, accredited Continuing Medical Education (CME) courses that focus on vector-borne and environmental illness within a One Health framework. These courses are available to clinicians and the public. To donate to this initiative and to learn about Invisible International, please go here.
Reference:
Alruwaili, Y., Jacobs, M. B., Hasenkampf, N. R., Tardo, A. C., McDaniel, C. E., & Embers, M. E. (2023). Superior efficacy of combination antibiotic therapy versus monotherapy in a mouse model of Lyme disease. Frontiers in Microbiology, 14, 1293300. https://doi.org/10.3389/fmicb.2023.1293300
Invisible’s newest CME course, “Leptospirosis: A Clinical Perspective,” provides medical professionals with comprehensive knowledge about diagnosing and managing leptospirosis. Leptospirosis is the world’s most common zoonotic disease, which is a category defined by infections that are spread between people and animals. It is often transmitted to humans through contaminated water. Taught by Dr. D. Scott Smith, a Stanford-trained infectious disease physician, the course draws from his extensive field experience. Dr. Smith has served as the Chief of Infectious Disease and Geographic Medicine at Kaiser Redwood City in California and is a current co-chair on the Professional Education Committee in the International Society of Travel Medicine.
Dr. Smith highlights the critical nature of leptospirosis. “Prompt recognition and appropriate management of this disease are crucial for clinicians, as it can be life-saving,” he notes, emphasizing the importance of timely and accurate response to potential cases (1).
The course addresses leptospirosis as a global threat that frequently mimics diseases like Lyme disease. It is designed to improve healthcare providers’ ability to identify the often non-specific symptoms of leptospirosis, which often pose a challenge in its early detection.
A key component of the course is the One Health approach, which melds human, animal, and environmental health considerations. This is crucial for the comprehensive understanding and management of leptospirosis.
Participants will delve into the diagnostic challenges of leptospirosis and explore the limitations of current testing methods. Treatment and prevention protocols, focusing on antibiotics such as doxycycline and penicillin, are covered. Strategies for avoiding exposure to contaminated environments such as stagnant bodies of water and lakes, and the use of appropriate protective gear are emphasized to limit the spread of leptospirosis. Under Dr. Smith’s guidance, this course aims to equip healthcare professionals with essential insights and practical skills to effectively confront leptospirosis, enhancing their capacity to address this significant global health challenge
The Invisible Education Initiative, funded by the Montecalvo Foundation, provides free, accredited Continuing Medical Education (CME) courses that focus on vector-borne and environmental illness within a One Health framework. These courses are available to clinicians and the public. To donate to this initiative and to learn about Invisible International, please go here http://invisible.international/give.
National Center for Biotechnology Information: Leptospirosis Overview. (Link)
Invisible is dedicated to ensuring that no Lyme+ patient is left behind. We focus on educating physicians about vector-borne diseases, and our efforts are entirely fueled by the generous support of donors like you.
Your contribution can help us expand our reach to more doctors and develop new educational courses.
Thank you for your commitment to helping us make a difference.
As we approach Giving Tuesday, a day dedicated to generosity and philanthropy, I urge you to consider the critical work of Invisible International. The shortage of trained providers in this field is worsening, a concern highlighted by the alarming statistics reported by the Centers for Disease Control:
Diseases spread by mosquitoes, ticks, and fleas tripled in the U.S. from 2004 to 2016.
Nine new pathogens spread by these vectors have been discovered since 2004.
Annually, 476,000 Americans are diagnosed with Lyme disease across all 50 states.
Despite these daunting figures, a 2023 study led by Cornell University revealed a stark reality: there is a limited availability of continuing education for life-threatening tick-borne diseases in the United States. (1) Another study revealed that the biggest barrier to patient access to treatment for Lyme disease is lack of physician education. (2)
Invisible International stands at the forefront of addressing this educational gap. We have created 40 CME courses for physicians, impacted over 100 institutions, delivered medical education presentations at 5 conferences, developed 3 clinical guides, and through our educational efforts, we have reached physicians who deliver vector-borne disease awareness to over 1,500,000 patient visits. Our courses, accredited by the Accreditation Council for Continuing Medical Education (ACCME) and reviewed by the American Academy of Family Physicians (AAFP), cover crucial aspects such as prevention, diagnosis, and treatment. These courses are available at no cost online, ensuring accessibility for all who need them.
Our initiative is further strengthened by the support of the Montecalvo Foundation, enabling us to offer these vital resources freely. However, to continue and expand our work, we rely on the generosity of individuals like you. Your donations empower us to educate more healthcare providers, enhance disease awareness, and ultimately save lives.
On this Giving Tuesday, I ask you to join us in this trailblazing mission, ensuring no patient is left behind. Your contribution will directly impact the fight against vector-borne diseases and support healthcare professionals in providing the best possible care to those affected.
On behalf of all of us at Invisible,
with gratitude,
Dr. Nev Zubcevik
Chief Medical Officer
Invisible International
References:
Malkowski AC, Smith RP, MacQueen D, Mader EM. Review of Continuing Medical Education in Tick-Borne Disease for Front-Line Providers. PRiMER. 2023;7:497812. Published 2023 Feb 2. (doi:10.22454/PRiMER.2023.497812)
Johnson LB, Maloney EL. Access to Care in Lyme Disease: Clinician Barriers to Providing Care. Healthcare. 2022; 10(10):1882. (https://doi.org/10.3390/healthcare10101882)
In our new course, “An Introduction to Human Babesiosis,” you’ll learn how to diagnose and treat infections caused by babesia, a malaria-like protozoan parasite that can be transmitted through tick bites, blood transfusions, and organ transplants, or congenitally from mother to fetus. The course is taught by Elizabeth Maloney, MD, the Education Co-director at Invisible, a Minnesota family physician, and the founder/president of Partnership for Tick-borne Diseases Education, a nonprofit providing evidence-based education on tick-borne diseases.
The disease parasite babesia, called babesiosis, lives in red blood cells. It was originally found only in cattle. It crossed over to humans in Croatia in 1956 and in Colorado and Massachusetts in the late 1960s. [1] Recent studies show that this parasite is more prevalent than previously thought, with Babesia microti being found in 1-in-10 of the ticks in southern New England and up to 15% of ticks in Suffolk County (Long Island), New York. [2]
When ticks transmit both Lyme disease and babesia simultaneously, patients are sicker and the resulting disease is harder to treat. [3] Coinfected patients are more likely to have fatigue, headaches, sweats, chills, anorexia, emotional lability, nausea, conjunctivitis, and splenomegaly more frequently than those with Lyme disease alone. The disease can be fatal for patients with damaged or missing spleens.
The course also discusses the global distribution of babesia and a new species of babesia, B. odocoilei, which may be causing unrecognized disease.
“Babesiosis is an emerging infectious disease yet many clinicians have had no or very little training about it. This can lead to missed diagnoses and increased morbidity for patients.” said Dr. Maloney, “unrecognized cases of babesiosis in blood donors have produced transfusion-transmitted cases which carry a significant mortality risk. Informing clinicians about the infection will ultimately improve patient care. The primary goal of this CME offering is for clinicians to include babesiosis in their differential diagnosis, when clinically appropriate.”
The Invisible Education Initiative, funded by the Montecalvo Foundation, provides free, accredited Continuing Medical Education (CME) courses that focus on vector-borne and environmental illness within a One Health framework. These courses are available to clinicians and the public. To donate to this initiative and to learn about Invisible International, please go here http://invisible.international/give.
References
Hildebrandt A, Zintl A, Montero E, Hunfeld KP, Gray J. Human Babesiosis in Europe. Pathogens. 2021 Sep 9;10(9):1165. doi: 10.3390/pathogens10091165. PMID: 34578196; PMCID: PMC8468516. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8468516/
From the Desk of Dr. Nev Zubcevik A letter to our supporters from Dr. Nev Zubcevik, Chief Medical Officer, on a new clinical tool that will help doctors better understand & care for patients with neurological Lyme disease. Dear community members and supporters,
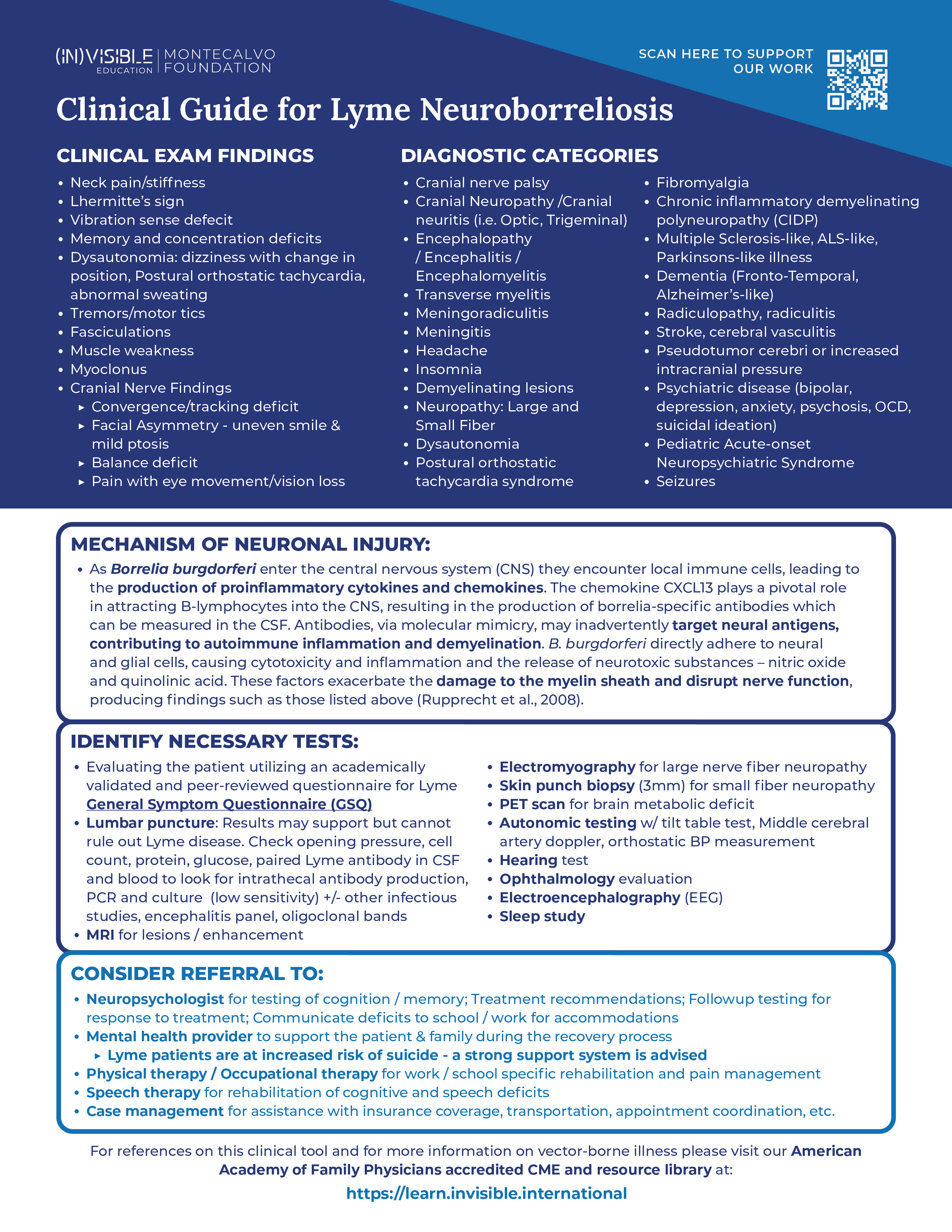
As a physical medicine and rehabilitation physician, my primary focus is on identifying the root cause of my patients’ illnesses. Only by addressing the underlying cause can we effectively rehabilitate our patient’s injuries. Throughout my years of practice, I have witnessed the devastating impact of untreated or under-treated Lyme disease infection on patients’ nervous systems. This destructive effect severely impairs their cognitive abilities, physical functioning, and overall quality of life. Our team at Invisible International has developed a clinical guide to assist clinicians in the recognition of neurological Lyme disease symptoms and subsequent diagnostic, testing, and treatment strategies to help diagnose and treat patients faster. We are grateful to donors like you who help fuel our work to pave the way for making sure every physician is a Lyme+ knowledgeable physician. To partner with us in developing and disseminating our education to physicians, please consider a tax-deductible donation today.
Lyme patients are at an increased risk of suicide
My deepest concern as a physician is that Lyme patients are extremely vulnerable as a population. Research has shown that Lyme patients face a heightened risk of suicide, primarily because their neurological injury remains largely invisible, causing immense suffering (Fallon et al., 2021). Understanding the clear mechanism of injury caused by the Lyme bacterium is crucial in explaining this invisible damage. By raising awareness among physicians and healthcare professionals about this mechanism, we can approach these patients with a clearer path to diagnosis and treatment.
Our study shows damage to the nervous system
In 2019, our team at Harvard conducted research and published the study “Association of Small Fiber Neuropathy and Post Treatment Lyme Disease Syndrome,” where we investigated the potential link between small fiber neuropathy (SFN) and post-treatment Lyme disease syndrome (PTLDS). Our findings provided both a biomarker of injury and a testing protocol that other physicians can use to objectify their patients’ neurological injury caused by Lyme disease.
In the study, we explored ten participants with a history of PTLDS, and through skin biopsies, we discovered evidence of SFN in all cases. Specifically, nine participants displayed sensory SFN with abnormal epidermal nerve fiber density, and seven individuals exhibited severe SFN. We observed autonomic dysfunction in all PTLDS participants. Additionally, our study revealed reduced cerebral blood flow in all PTLDS patients, suggesting cerebral hypoperfusion.
Our findings suggest that SFN and related dysautonomia may serve as objective markers for PTLDS. The assessment of small fiber density and autonomic dysfunction using skin biopsies and reflex testing could be valuable in therapeutic trials and offer physicians a clearer understanding of PTLDS and its associated symptoms, including cognitive impairment and brain fog.
The mechanisms like direct cytotoxicity by the spirochete, neurotoxic mediators during host-pathogen interactions, and triggered autoimmune reactions are likely to be involved in the pathogenesis of this neuronal injury.
The mechanism of neuronal injury in Lyme is clear
The article “The Pathogenesis of Lyme Neuroborreliosis: From Infection to Inflammation” by Rupprecht et al. (2008) is a crucial source of information that sheds light on the intricate mechanism of neuronal injury in Lyme disease. Lyme neuroborreliosis, caused by the spirochete Borrelia burgdorferi, can lead to neurological manifestations, including painful meningoradiculitis and cranial or peripheral neuritis. Understanding the pathogenesis of this condition is essential for effective management and treatment.
The infection process begins with the spirochetes entering the tick’s salivary glands during feeding and subsequently invading the host’s skin, leading to a local infection called erythema migrans. During the second stage of Lyme disease, the spirochetes can spread to various organs, including the central nervous system (CNS), resulting in neurological complications.
The spirochetes employ various strategies to evade the host’s immune system. They downregulate immunogenic surface proteins, such as OspA and OspC, to minimize their recognition by immune cells. Additionally, they express complement-neutralizing proteins and induce anti-inflammatory cytokines to suppress the host’s immune response. These mechanisms enable the spirochetes to establish infection and persist in the host.
Once the spirochetes enter the CNS, they encounter local immune cells, leading to the production of proinflammatory cytokines and chemokines. The chemokine CXCL13 plays a pivotal role in attracting B-lymphocytes into the cerebrospinal fluid (CSF), resulting in the production of borrelia-specific antibodies. This immune response, however, can also contribute to the neuronal injury.
The neurological dysfunction observed in Lyme neuroborreliosis may result from multiple factors. The spirochetes can directly adhere to neural and glial cells, causing cytotoxicity and inflammation in the surrounding tissues. Furthermore, they induce the release of neurotoxic substances, such as nitric oxide and quinolonic acid, exacerbating the damage. Additionally, the immune response may lead to an autoimmune reaction, with antibodies targeting neural antigens due to molecular mimicry, further contributing to inflammation and demyelination.
The demyelination process is particularly significant as it can disrupt nerve function and result in various neurological symptoms. Damage to the myelin sheath, the protective covering of nerve fibers, can lead to muscle weakness, numbness, tingling, and coordination difficulties.
What we are doing and how you can help
The mechanisms discussed, including immune evasion, inflammation, and demyelination, contribute to the complex clinical picture of this condition. Understanding these processes is crucial for developing targeted therapies to mitigate nerve injury and promote recovery in patients with Lyme neuroborreliosis. We must do better to educate the medical system about this mechanism of injury. With this information, the stigma will disappear, and the patients will be listened to and treated properly. Insurance companies will follow this by covering treatments.
Education leads to meaningful and lasting change. And we are paving the way.
Just in the last 6 months, we have educated physicians via the Montecalvo Education Platform for Vector-Borne Illness to impact over 750,000 patient visits. Our virtual courses have been viewed over 14,000 times. This work is only possible with your support: we rely on gifts from donors like you to make sure no Lyme patient is left behind. Your donations help us expand programming, send our team to conferences, and help us develop educational guides. Please consider making your tax-deductible donation today.
From all of us here at Invisible, With gratitude,
Nevena Zubcevik, DO Chief Medical Officer Invisible International
References:
Fallon BA, Madsen T, Erlangsen A, Benros ME. Lyme Borreliosis and Associations With Mental Disorders and Suicidal Behavior: A Nationwide Danish Cohort Study. Am J Psychiatry. 2021 Oct 1;178(10):921-931. doi: 10.1176/appi.ajp.2021.20091347. Epub 2021 Jul 28. PMID: 34315282.
Novak P, Felsenstein D, Mao C, Octavien NR, Zubcevik N. Association of small fiber neuropathy and post treatment Lyme disease syndrome. PLoS One. 2019 Feb 12;14(2):e0212222. doi: 10.1371/journal.pone.0212222. PMID: 30753241; PMCID: PMC6372188.
Rupprecht TA, Koedel U, Fingerle V, Pfister HW. The Pathogenesis of Lyme Neuroborreliosis: From Infection to Inflammation. Mol Med. 2008 Nov-Dec;14(11-12):205-12. doi: 10.2119/2007-00091.Rupprecht. PMID: 18787810; PMCID: PMC2270991.
As you all are aware, the treatment of patients suffering from tick-borne diseases can be quite complicated. However, a research article published in Antibiotics (June 2023) by Trouillas and Franck (1) offers an encouraging method for addressing the severe neurological symptoms associated with these diseases. They observed full recovery in seven out of ten patients with severe neurological Lyme disease, marked by paresis. Importantly, these patients stayed healthy even two years after recovery.
Patients in this study had been dealing with their illnesses for periods ranging from six months to seven years. None had been treated with antimicrobials. The researchers scrutinized several recognized, but under-researched, problems within the field.
Their findings contradicted the existing recommendation to treat neuroborreliosis with 21 days of a single drug, Ceftriaxone. Out of 16 treatment studies focused on patients with Neurologic Lyme, only 15 individuals could be diagnosed as having late-stage Lyme neuroborreliosis. Interestingly, studies employing long-term antibiotics showed better outcomes for patients (2,3,4).
A key aspect of their research was the consideration of patients suffering from multiple tick-borne diseases simultaneously, such as Borrelia, Babesia, Bartonella, and Anaplasma.
Patients were treated until their neurological symptoms disappeared. If symptoms recurred after a period of remission, treatment was resumed and continued until remission could again be achieved.
In line with this, the researchers treated patients for Lyme disease (Borreliosis) and other co-infections such as Babesiosis, Bartonellosis, and Anaplasmosis, if a patient’s symptoms and lab tests suggested the presence of these diseases. They used a combination of clinical judgment and lab testing to guide their treatment decisions. They also referred to studies suggesting the persistence of these infections, which justified the need for prolonged antimicrobial treatment.
Treatment continuation was decided based on the patient’s clinical response, emphasizing a patient-centric approach. The results were significant: seven out of ten patients regained their health, allowing them to resume societal and family roles, without previous discomfort. On average, treatment duration needed to achieve this was 25 months. This study represents a promising development in the management of severe tick-borne diseases, although more research is needed to validate and apply these findings more broadly.
Patients who suffer with tick-borne diseases need faster research results that translate to meaningful clinical interventions and better outcomes. A solution to this is Invisible’s Tick Bytes Clinical Data Repository. This is an initiative to organize clinical information from the ten best tick-borne disease physicians across the nation within a privacy-protected database, enabling researchers to analyze and publish best practices for treating patients.
With this precision medicine approach, more quality evidence will reach physicians, insurers, and the government, leading to better patient outcomes, insurance coverage, and a deeper understanding of tick-borne diseases.
Based on prior work by Dr. Nevena Zubcevik and Dr. Charlotte Mao at the Dean Center for Tick Borne Illness in Boston, it’s anticipated that it will take 12 months for database set-up, and 24 months for data collection, analysis, and publication. To move forward, all we need is funding from people like you. Please help us launch this important initiative.
References:
Trouillas P, Franck M. Complete Remission in Paralytic Late Tick-Borne Neurological Disease Comprising Mixed Involvement of Borrelia, Babesia, Anaplasma, and Bartonella: Use of Long-Term Treatments with Antibiotics and Antiparasitics in a Series of 10 Cases. Antibiotics (Basel). 2023 Jun 7;12(6):1021. doi: 10.3390/antibiotics12061021. PMID: 37370340; PMCID: PMC10294829.
Logigian EL, Kaplan RF, Steere AC. Successful treatment of Lyme encephalopathy with intravenous ceftriaxone. J Infect Dis. 1999 Aug;180(2):377-83. PMID: 10395852 DOI: 10.1086/314860
Oksi, J.; Kalimo, H.; Marttila, R.J.; MariamaÃàki, M.; Sonninen, P.; Nikoskelainen, J.; Villanen, M.K. Inflammatory brain changes in Lyme borreliosis. A report on three patients and review of literature. Brain 1996, 119 Pt 6, 2143-2154. https://doi.org/10.1093/brain/119.6.2143
Fallon, B.A.; Keilp, J.G.; Corbera, K.M.; Petkova, E.; Britton, C.B.; Dwyer, E.; Slavov, I.; Cheng, J.; Dobkin, J.; Nelson, D.R.; et al. A randomized, placebo-controlled trial of repeated IV antibiotic therapy for Lyme encephalopathy. Neurology 2008, 70, 992–1003. DOI: https://doi.org/10.1212/01.WNL.0000284604.61160.2d
A Massachusetts General Hospital study that raises the awareness of possible cardiac involvement in early Lyme patients was recently published. This small study is the first to use data that measures a complex protein (troponin) to detect possible cardiac involvement in patients with early Lyme disease and with subclinical, or non-noticeable cardiac symptoms. Overall, 14.6% of the study subjects had elevated troponin T levels above the normal range. These findings were published in the March 2022 issue of Annals of Clinical & Laboratory Science and are explained in a new course from Invisible International, taught by first author Elizabeth Lee Lewandrowski, PhD, MPH, an Assistant Professor of Pathology at Harvard Medical School, a Faculty Researcher and Clinical Laboratory Scientist in Pathology at Massachusetts General Hospital, and Invisible International’s Research Director.
Troponin is a complex of three proteins (troponin T, I, and C) that regulate muscle contractions in the heart. When the heart is damaged, these proteins are released into the bloodstream, allowing clinicians to measure levels to determine the extent of heart damage. Both troponin T and I are detected and elevated in the blood when the heart is negatively impacted by various conditions, including infection, inflammation, or muscle damage. Therefore, this is potentially an important test for doctors to follow in the event of suspected cardiac involvement including subclinical cardiac involvement in patients with Lyme disease.
Previously, the Centers for Disease Control and Prevention reported that Lyme carditis occurs only in about 1% of Lyme disease cases (2008 to 2017). This newer study of 41 early Lyme patients used the high sensitivity troponin T test and found that 14.6% had elevated troponin T levels, suggesting that the heart is damaged in more early Lyme disease cases than previously realized. This finding should be brought to the attention of healthcare providers as it suggests cardiac involvement in early Lyme disease may be more common than previously realized. While there are many explanations for elevated troponin levels in these patients, including a systemic inflammatory response, this result raises the question that subclinical cardiac involvement may be more common than previously recognized. Further investigation is necessary to explore and validate the significance of this finding.
Some of the heart conditions that troponin T tests can detect include electrical disruptions (AV block, most common in Lyme carditis), inflammation (myocarditis), swelling of the heart sac (pericarditis), inflammation of the inner lining and valves (endocarditis), problems with the pumping action (cardiomyopathy), and heart attacks (myocardial infarctions). Some of these conditions can be fatal, emphasizing the need for rapid diagnosis and treatment when Lyme carditis is suspected.
The Invisible Education Initiative, funded by the Montecalvo Foundation, provides free, accredited Continuing Medical Education (CME) courses that focus on vector-borne and environmental illness within a One Health framework. These courses are available to clinicians and the public. To donate to this initiative and to learn about Invisible International, please go here http://invisible.international/give.
If you’re a clinician looking for new evidence-based insights into diagnosing Lyme disease, this course is a good starting place. It begins with a brief overview of the One Health approach to combating vector-borne diseases. Then it applies this framework to Lyme disease, which accounted for 60% of all vector-borne diseases in the U.S. from 2004 to 2016.
Early Lyme diagnostic strategies are addressed by Elizabeth Maloney, MD, the Education Co-director at Invisible, a Minnesota family physician, and the founder/president of Partnership for Tick-borne Diseases Education, a nonprofit providing evidence-based education on tick-borne diseases. Dr. Malone reviews four cases that highlight symptom patterns to look for in diagnosing early Lyme, Lyme carditis, and cranial neuritis, which often presents as facial Bell’s Palsy. She also discusses the flaws inherent in current Lyme diagnostic tests.
Late-stage Lyme disease rehabilitation is covered by Nevena Zubcevik, DO, Chief Medical Officer of Invisible International, previously co-founder and co-director of the Dean Center for Tick Borne Illness at the Spaulding Rehabilitation Hospital, an affiliate of Harvard Medical School. Dr. Zubcevik emphasizes that Lyme diagnostics aren’t always reliable for late-stage Lyme, so she presents evidence-based symptom clusters that may help clinicians with diagnoses. To assess the nervous system inflammation that is characteristic of late Lyme, she recommends taking a punch biopsy to test for small fiber neuropathy, and PET brain scans to confirm the inflammation that is at the root of the memory deficits found in 74% of these patients.
In addition to this course, Invisible offers resources to help in clinicians in the diagnostic process. These include a General Symptom Questionnaire (GSQ-30) for assessing patient impairment; a health risk assessment tool that helps patients think about exposures to environmental, animal, and travel-related diseases that might be contributing to ill health; and an evidence-based symptom list for babesiosis, bartonellosis and (Lyme) borreliosis, all common tick-borne diseases.
Invisible International is developing courses and clinician tools like these to accelerate the movement of new research to frontline clinicians. We hope these anytime, anywhere courses will grow the pool of health-care providers who are experienced in the diagnosis and treatment of tick- and other vector-borne diseases. This means fewer patients will have to travel long distances and wait months for an initial appointment. Education heals.
The Invisible Education Initiative, funded by the Montecalvo Foundation, provides free, accredited Continuing Medical Education (CME) courses that focus on vector-borne and environmental illness within a One Health framework. These courses are available to clinicians and the public. To donate to this initiative and to learn about Invisible International, please go here http://invisible.international/give.
There’s a dire shortage of health-care providers who are experienced in the diagnosis and treatment of tick- and other vector-borne diseases. This means many suffering patients must travel long distances and wait months for an initial appointment, leading to worse patient outcomes. [1]
There are immense insurance and logistical barriers that discourage providers from taking on patients with tick-borne diseases. Some of these were identified in a 2022 survey-study of 155 clinicians from 30 states who treat Lyme patients. They included complexity of care (79%), the cognitive impairment of patients (57%), and frequent patient calls between scheduled appointments (49%). [1]
This shortage of trained providers is getting worse as the incidence of vector-borne diseases rises. The Centers for Disease Control reports that:
Diseases spread by mosquitoes, ticks, & fleas tripled in the U.S., 2004-2016.
Since 2004, 9 new pathogens spread by mosquitoes & ticks have been discovered.
476,000 Americans are diagnosed with Lyme disease each year, in all 50 states.
Invisible International is filling this educational gap by producing best-in-class Continuing Medical Education (CME) courses on vector-borne and environmental disease, available to anyone online for no cost. These courses cover prevention, diagnosis, and treatment of these disease.
What is CME?
Continuing Medical Education (CME) educational activities are classes, workshops, or conferences that increase the knowledge and skills of health-care providers, ensuring that they stay current on the latest medical research and best medical practices. Some states require that doctors, nurses, and other health professionals accrue a certain number of CME course credits each year to keep their medical licenses active.
What is unique about its CME offerings?
Invisible has one of the largest online CME collections of vector-borne diseases available. The courses are delivered by some of the most knowledgeable experts in their respective fields, featuring topics like persistent Lyme disease, the Bartonelloses, Lyme disease treatment, and neuropsychiatric symptoms of tick-borne diseases. Our courses incorporate the One Health concept, a recognition that the health of humans, pets, and the environment are all intertwined.
What is CME accreditation?
CME courses can be developed by medical societies, universities, companies, or nonprofits such as Invisible International. For these activities to be counted towards annual CME totals, they must be approved by independent accreditation organizations. This ensures that the educational activities are relevant, practice-based, effective, based on valid content, and independent of commercial influence.
Is Invisible’s CME accredited?
Invisible International’s Continuing Medical Education (CME) platform is accredited by two governing bodies:
The Accreditation Council for Continuing Medical Education (ACCME) sets course development guidelines to ensure accurate, balanced, scientifically justified clinical-practice recommendations, all free of commercial bias.
communicate the risks and benefits of clinical recommendations
evaluate a learner’s grasp of the material.
Physicians taking AAFP-approved courses can receive reciprocal continuing education credits from the American Medical Association, (AMA), the American Osteopathic Association (AOA), the College of Family Physicians of Canada (CFPC), and other health professional organizations.
The Invisible Education Initiative, funded by the Montecalvo Foundation, provides free, accredited Continuing Medical Education (CME) courses that focus on vector-borne and environmental illness within a One Health framework. These courses are available to clinicians and the public. To donate to this initiative and to learn about Invisible International, please go here http://invisible.international/give.
###
[1] Johnson LB, Maloney EL. Access to Care in Lyme Disease: Clinician Barriers to Providing Care. Healthcare. 2022; 10(10):1882. https://doi.org/10.3390/healthcare10101882
The authors of this study are Elizabeth L. Maloney, MD, a Minnesota family physician and Invisible’s education co-director; and Lorraine Johnson, JD, MBA, the Chief Executive Officer of LymeDisease.org and the principal investigator of its patient registry and research platform, MyLymeData.
[2] Malkowski AC, Smith RP, MacQueen D, Mader EM. Review of Continuing Medical Education in Tick-Borne Disease for Front-Line Providers. PRiMER. 2023;7:497812. Published 2023 Feb 2. doi:10.22454/PRiMER.2023.497812