A retrospective study of 270 post-treatment Lyme patients identified the most debilitating neurological symptoms, paving the way for future studies on root causes of disease and better treatments.
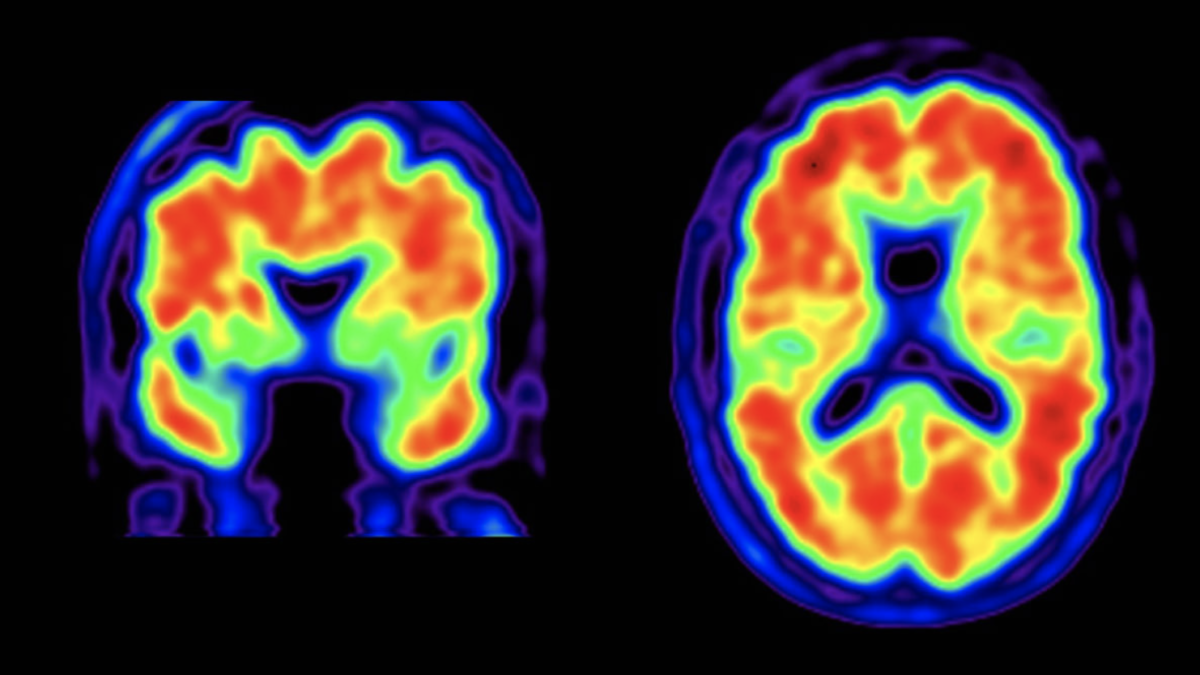
The largest study to-date characterizing ongoing symptoms [1] of Lyme patients after antibiotic treatment has been published by a group of investigators at Harvard-affiliated hospitals and Invisible International, a non-profit organization. They also examined the relationship between symptom severity and perceived disability, identifying five of the most debilitating symptom categories — fatigue, cognitive deficits, neuropathy (nerve numbness or weakness in the extremities), migraine headaches, and mood disorders.
The study lays a scientific foundation for future research that will help the growing ranks of post-treatment Lyme patients suffering from lingering symptoms. Lyme disease is the fastest vector-borne illness in the United States, with an estimated 476,000 new cases a year, according to the Centers for Disease Control. Approximately 10 to 36% [2] of those treated with antibiotics go on to experience disabling long-haul symptoms, such as severe fatigue, joint/muscle pain, cognitive problems, and neurologic symptoms.
Patient impairment was assessed through medical chart reviews of 270 individuals who had been treated for Lyme borreliosis through the Dean Center for Tick-Borne Illness at Spaulding Rehabilitation Hospital Boston, a Harvard affiliate, between 2015 and 2018. Symptom and disability data was also collected through scientifically validated questionnaires. Symptom clusters were defined as two or more symptoms occurring together, indicating that they might share the same triggering mechanism. This approach, used in other chronic conditions, such as cancer and inflammatory bowel disease, helps guide researchers in identifying root causes and better treatment strategies.
“This study is an important first step in figuring out why these patients aren’t getting better,” said Dr. Nevena Zubcevik, DO, the first author on the study and the former co-director of the Dean Center for Tick Borne Illness. “Going forward, we’re taking what we’ve learned to set up a multi-institutional clinical data repository that will provide high quality, de-identified tick-borne illness patient data to any interested researcher.”
To expedite the discovery of clinical treatments for patients suffering with chronic tick-borne illness, Dr. Zubcevik is now leading the Tick Bytes Clinical Data Research Platform through Invisible International, in her role as Chief Medical Officer. The resulting open-source data would enable researchers to access prospectively acquired clinical and laboratory data, as well as possible biorepository specimens, on a large group of well-defined pediatric and adult patients with complex Lyme disease. This repository would also collect data on mixed infections and/or environmental/toxic exposures, influences that often worsen the outcomes of these patients. Using this precision-medicine approach, more quality evidence will reach physicians, insurers, and government. This, in turn, will improve diagnostics and treatment options, leading to better outcomes, insurance coverage, and government funding. Invisible is currently raising funds to launch 10 data collection sites at research institutions, community clinics, and hospitals across the nation.
Invisible International, a 501(c)(3) nonprofit organization, is dedicated to reducing the suffering and social marginalization associated with invisible illnesses through innovation, education, and data-driven change projects. Invisible’s core team includes board-certified health-care providers in Infectious Disease, Internal Medicine, Family Medicine, Psychiatry, Pharmacy, Pathology, and Physical Medicine and Rehabilitation, many trained at or are affiliated with top-tier universities such as Harvard, Stanford, MIT, Brown, UC Berkeley, UC San Francisco, the US Air Force Academy, University of Virginia, and University of Pittsburgh.
This study and Invisible International’s Change Platform for Tick-borne Illness were funded by generous donations from Mark and Eileen Lovell. The organization is currently seeking additional support to expand its TickBytes data collection sites. To learn more about how you can help, go to: https://invisible.international/give
You can sign up to receive news and updates at https://invisible.international/mission
###
Other related courses: Persistent Lyme disease, Neurologic complications of Lyme disease, Borrelia persistence “Bench to Bedside” E-Colloquium
Photo credit: francescoch/iStock
End Notes
[1]
Marques A. Chronic Lyme disease: a review. Infect Dis Clin North Am. 2008;22(2):341-viii. doi:10.1016/j.idc.2007.12.011
Asch ES, Bujak DI, Weiss M, Peterson MG, Weinstein A. Lyme disease: an infectious and postinfectious syndrome. J Rheumatol. 1994 Mar;21(3):454-61. PMID: 8006888. [Retrospective evaluation of 215 Lyme patients who were diagnosed and treated > 1 year prior. Found/described persistent symptoms in 114 (53%).]
Clarissou J, Song A, Bernede C, et al. Efficacy of a long-term antibiotic treatment in patients with a chronic Tick Associated Poly-organic Syndrome (TAPOS). Med Mal Infect. 2009;39(2):108-115. doi:10.1016/j.medmal.2008.11.012. [Open-label prospective study of 100 patients after treatment for chronic TAPOS (Tick Associated Poly-Organic Syndrome), evaluating their evolution on prolonged antibiotics.]
Horowitz RI, Freeman PR. Precision Medicine: The Role of the MSIDS Model in Defining, Diagnosing, and Treating Chronic Lyme Disease/Post Treatment Lyme Disease Syndrome and Other Chronic Illness: Part 2. Healthcare. 2018; 6(4):129. https://doi.org/10.3390/healthcare6040129. [Patient symptom survey and retrospective chart review of 200 patients with chronic Lyme/PTLDS.]
[2]
Strle, F., Cimperman, J., Maraspin, V. et al. Azithromycin versus doxycycline for treatment of erythema migrans: Clinical and microbiological findings. Infection 21, 83–88 (1993). https://doi.org/10.1007/BF01710737. [“Minor” symptoms in 15/52 (29%) who received doxycycline and 10/55 (18%) who received azithromycin.]
Dattwyler, R.J.; Luft, B.J.; Kunkel, M.J.; Finkel, M.F.; Wormser, G.P.; Rush, T.J.; Grunwaldt, E.; Agger, W.A.; Franklin, M.; Oswald, D.; et al. Ceftriaxone compared with doxycycline for the treatment of acute disseminated Lyme disease. N. Engl. J. Med. 1997, 337, 289–294. [Persistent symptoms at last follow-up visit in 18/68 (26%) Ceftriaxone vs 10/72 (13.9%) doxycycline.]
Aucott JN, Rebman AW, Crowder LA, Kortte KB. Post-treatment Lyme disease syndrome symptomatology and the impact on life functioning: is there something here?. Qual Life Res. 2013;22(1):75-84. doi:10.1007/s11136-012-0126-6. [Prospective cohort study of 63 patients with EM rash and systemic symptoms treated with doxycycline reported a 36% rate of PTLDS.]