The tick-borne disease epidemic in Ireland: A call for more research
In our newly released medical education course, a Dublin-based infectious disease physician-researcher raises the alarm about the undercounting and under-treatment of tick-borne diseases in Ireland, as well as the risk that this poses to the country’s blood supply.
This course, “Call for international collaboration and data sharing from the clinical trenches,” is taught by Jack Lambert, MD, PhD, a Professor of Medicine and Infectious Diseases at Mater and Rotunda hospitals, and University College of Dublin School of Medicine in Dublin, Ireland. He is also the founder of the Lyme Resource Centre in Scotland and a member of Invisible’s Scientific Advisory Board.
In the course, Dr. Lambert cites studies that have found that:
- The standard two-tiered antibody tests miss more than 50% of verifiable Lyme patients.
- One-in-five serum samples from the Irish blood bank showed the presence of antibodies to the Lyme disease bacterium, Borrelia burgdorferi. [Source: Irish Surveillance Center data from high prevalence areas]
- The overall rate of borrelial infection in ticks collected at six sites in Ireland was 5%, with a range from 2% to 12%, depending on the locations of tick collection. The most prevalent species detected were garinii (70%) followed by B. valaisiana (20%) and B. miyamotoi (10%). All of these Borrelia species cause human disease, and this is the first time that B. miyamotoihas been detected in Ireland.
“Most people don’t remember a tick, many don’t get the bullseye rash, and many are not offered a Lyme test. For those truly infected, the Lyme antibody test is insensitive. Until we have enhanced surveillance of clinical cases and improved sensitivity of the diagnostic testing, numbers of cases of Lyme disease and coinfections will be underreported,” said Dr. Lambert.
Dr. Lambert also highlights a major flaw in the Lyme disease tracking in Ireland: Reporting is only required for the most serious neurological manifestations of the disease, i.e., patients who have been admitted to a hospital and have had a lumbar puncture that shows specific abnormalities in the cerebral spinal fluid.
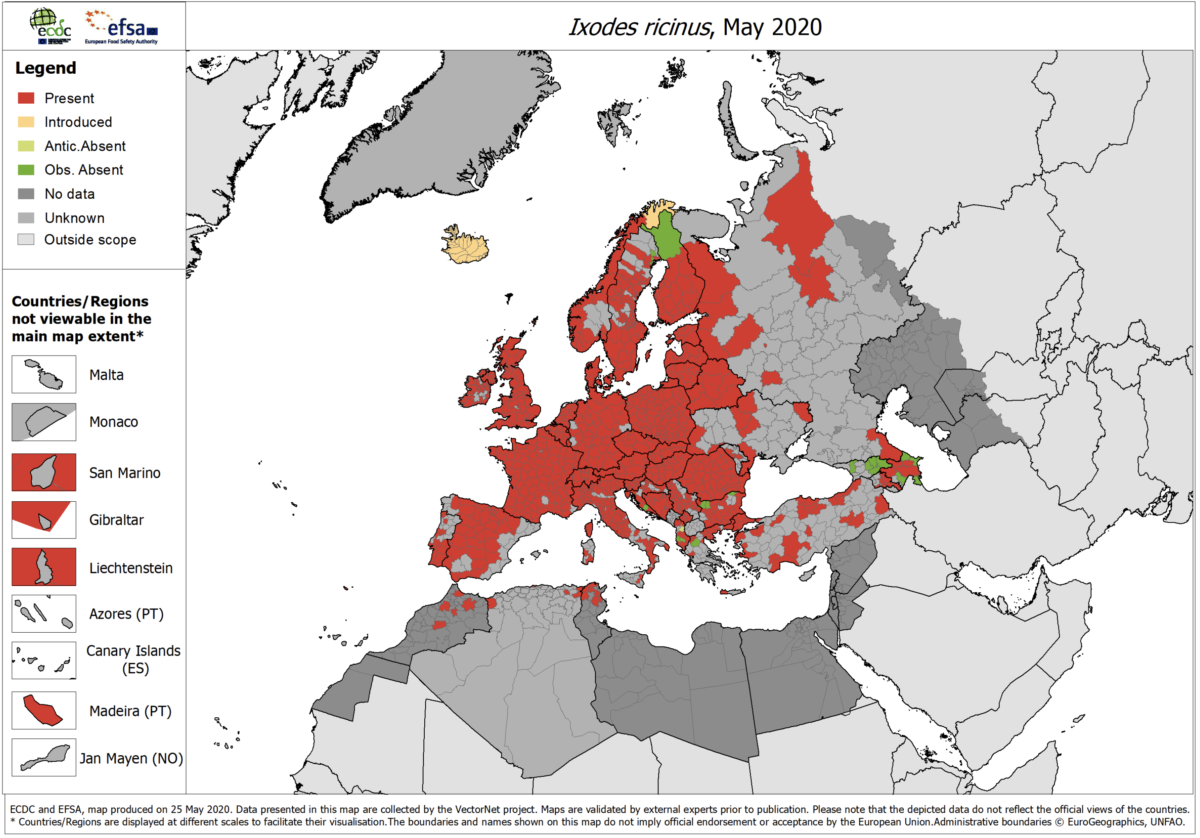
Other topics covered include the undercounting of Lyme cases in Canada and the United Kingdom, the geographic spread of Lyme in Europe, and the need to treat patients according to symptoms, not one-size-fits-all guidelines. He goes on to cite evidence that treating with longer courses of combinations of antibiotic yields better patient results.
This free, accredited Continuing Medical Education (CME) is brought to you by the Invisible Education Initiative, funded by the Montecalvo Foundation.
