Neuropsychiatric Lyme symptoms: A new masterclass
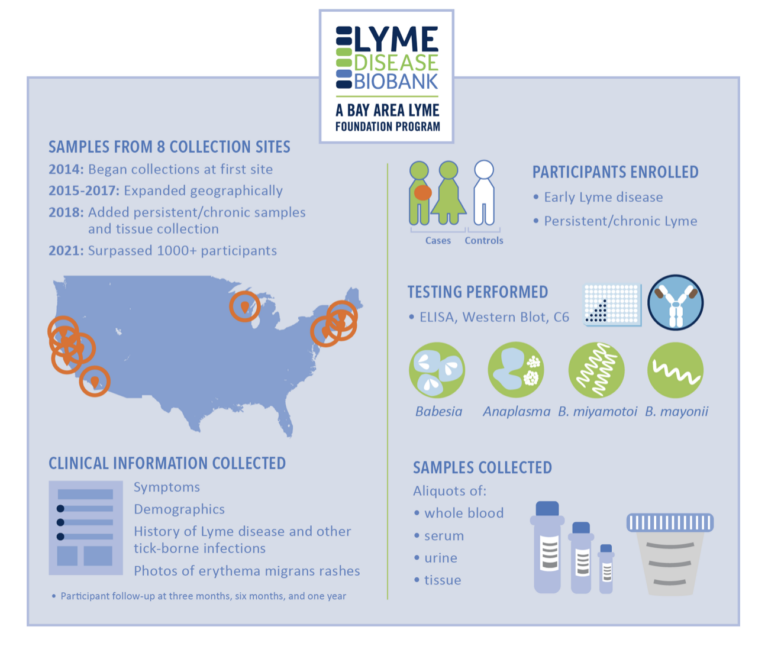
Invisible International has just released an important medical education course on neuropsychiatric symptoms associated with Lyme…

Invisible International has just released an important medical education course on neuropsychiatric symptoms associated with Lyme…

In the first study of its kind, two Lyme disease experts gathered data on a question…
Donating the tissues of a loved one who dies of Lyme disease is one of the…

A Dublin-based infectious disease doctor who’s treated both long COVID and chronic Lyme patients shares new…

Lyme disease affects children more than any other age group, but the young ones are often…
Dr. Nevena Zubcevik, co-founder of “The Dean Center for Tick Borne Illness” at Spaulding Rehabilitation Hospital/Harvard…

Whoever saves a life, it is considered as if he saved an entire world. —Mishnah Sanhedrin…

This week Invisible International shines a light on recent progress in the Lyme disease world with…
In 2019, the late-great-science-writer Sharon Begley wrote an insightful article, “The maddening saga of how an…

In this free medical education course, Kenneth Liegner, MD, a New York-based internist who has been…
End of content
End of content